
Anti-Black Racism and Schizophrenia: Past and Present
/“There are forces of nature and circumstance that are beyond our control, let alone our understanding, and to insist on victory in the face of this, to accept nothing less, is just asking for a soul-pummeling. The simple truth is, not every fight can be won”
Schizophrenia is a long-term mental disorder that can manifest in symptoms such as delusions, hallucinations, disorganized speech, trouble with thinking and lack of motivation. For people like Elyn Saks, who has lived with schizophrenia for much of her life, this mental disorder is truly all-encompassing. Although the purpose of a diagnosis with schizophrenia (or any mental illness) is ideally to provide care and treatment, diagnosis with schizophrenia or “insanity” has been used to oppress Black people. Moreover, the legacy of these racist psychological practices lives on in modern-day psychiatry.
Here, we will explore the ways in which anti-Black racism has been and continues to be infused into the definition and diagnosis of schizophrenia. We will first learn about the historical ways that a diagnosis of “insanity” was used to oppress and discredit Black Americans in the 1800s and then during the civil rights movement of the 1960s. Then, we will dive into modern-day issues surrounding diagnosis and treatment of schizophrenia in Black individuals.
“Psychologically Unfit for Freedom”
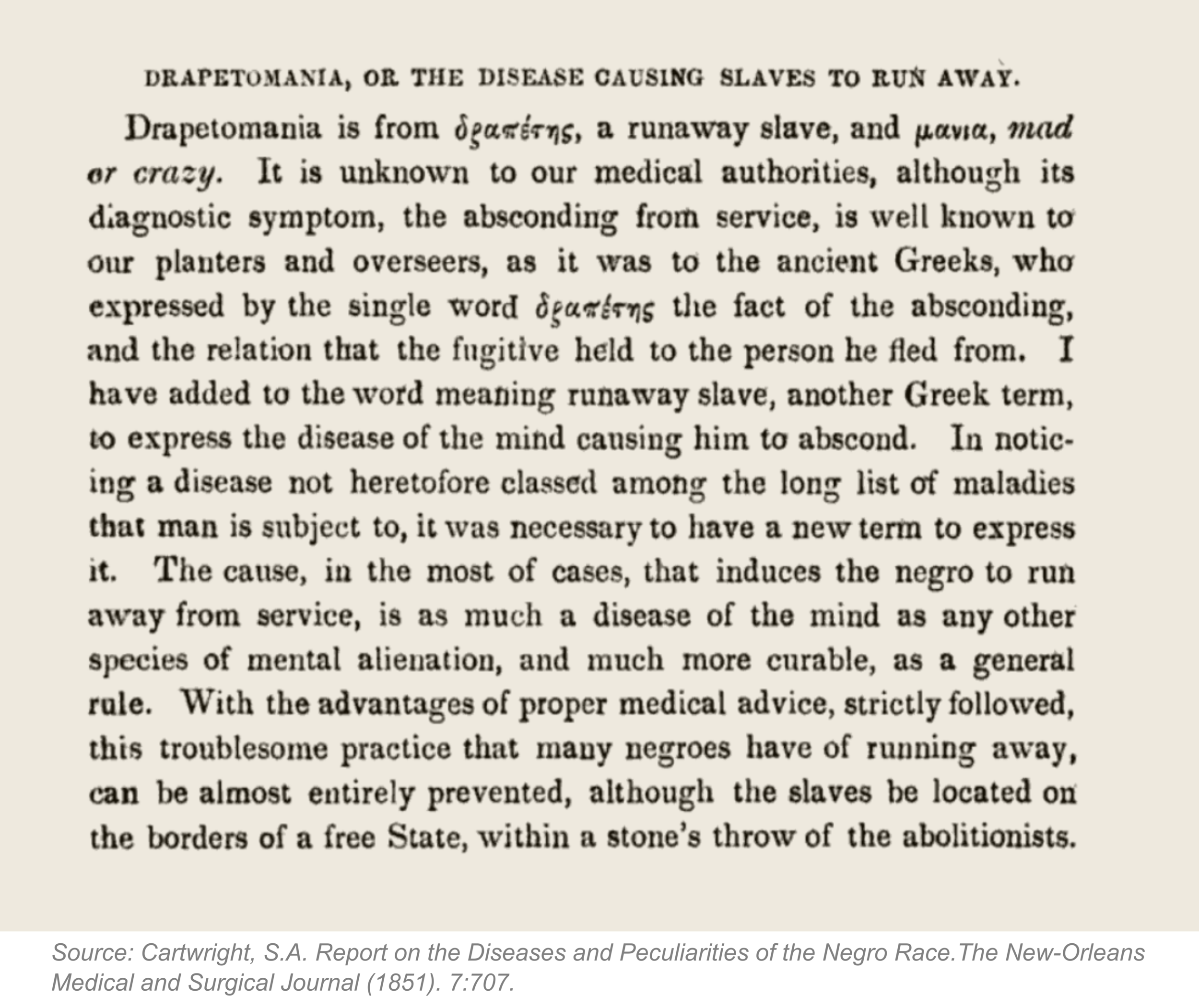
Our story begins in the 1850s, when American psychiatrists used insanity to justify the enslavement of Black people. Samuel Cartwright, a Louisiana surgeon and psychologist, conjured up a mental illness he called “drapetomania,” which he claimed drove enslaved Black individuals to flee from captivity. Cartwright claimed that this disorder was caused by slave owners making “themselves too familiar with the slaves, treating them as equals.” Drapetomania, shockingly, remained in the Practical Medical Dictionary until 1914.
In addition to drapetomania, Cartwright also described “dysaesthesia aethiopica,” a mental illness which he claimed was the supposed root of laziness, “rascality” and “disrespect for the master’s property” in Black enslaved people. According to Cartwright, this illness was caused by lesions or insensitivity of the skin and caused “so great a hebetude [mental dullness or lethargy] of the intellectual faculties, as to be like a person half asleep.” It was thought that this condition was more prevalent among free Black Americans. Even at the turn of the twentieth century, American psychiatrists claimed that Black enslaved people were “psychologically unfit for freedom.” Because scientific principles are considered to be “objective truths” by the rest of society, the formalization of “conditions” such as drapetomania or dysaesthesia added credence to the idea that Black people were inherently inferior.
Protest Psychosis: Shifting Mental Health Diagnoses and Anti-Black Racism
These troubling and dangerous notions of the “psychological unfitness” of Black Americans morphed after the early twentieth century. Those in power continued to use insanity to silence Black voices speaking out against racial injustices. In his book The Protest Psychosis, Jonathan Metzl describes how schizophrenia was re-written as a “disease” of the Black protestor.
Prior to the civil rights movement in the 1960s, schizophrenia was predominantly diagnosed in white people, and those diagnosed with schizophrenia were characterized as docile and harmless. Patients with schizophrenia were commonly treated as “unruly children'' that could be nurtured by their psychotherapists. Of course, schizophrenia was never just a white disease; rather, American mainstream culture defined schizophrenia as a disease that only afflicted white people and systematically rendered other groups invisible.

This characterization of schizophrenia changed radically in the 1960s. Suddenly, leading medical sources described schizophrenia as a disease that affected Black men and manifested in rage, not docility. Psychiatrists of the 1960’s even went so far as to describe schizophrenia in Black men as “protest psychosis” characterized by “hostile and aggressive feelings” and “delusional anti-whiteness.” They claimed that such psychosis could develop if Black men listened to speeches by Malcolm X, joined the Black Muslims, or aligned with groups that “preached militant resistance to white society.” Even the advertisements for newly-developed pharmaceutical treatments for schizophrenia such as Haldol (see image on right) read like anti-Black propaganda, showing angry, Black men with their fists clenched at the reader. Schizophrenia, previously a mental illness like any other, was weaponized in the 1960s to both demonize and discredit Black protestors.
Medical practitioners were not the only ones characterizing Black protestors as mentally ill. Newspapers of the 1960s and 1970s routinely described schizophrenia as a sequela of angry, Black masculinity and warned readers of schizophrenic Black killers via outrageous headlines such as “FBI Adds Negro Mental Patient to ‘10 Most Wanted List.’” Popular movies also depicted Black men (and in particular Black civil rights activists) as mentally ill, as in the 1963 Shock Corridor.
These descriptions of “protest psychosis” bear some similarities to the ways in which today’s Black Lives Matter protests are sometimes described in the media. The language is eerily similar: these protests are “riots” characterized mainly by violence. This is just untrue; the data overwhelmingly supports that the vast majority of BLM protests were peaceful. So far in this article, we have explored our country’s fraught history of using insanity as a tool of oppression against Black people fighting for their liberation. We cannot continue to use this kind of language to describe Black people and Black-run organizations that stand against racism and oppression of Black people.
Where Do We Stand Today?
It might be tempting to cast these stories as purely historical. However, as Alvin Pouissant, a clinical professor of psychiatry at Harvard Medical School, reminds us in a New York Times interview, “The culture influences what you consider pathology. Cartwright saw slavery as normative. So when slaves deviated from the norm, he called them mentally ill. The business of deciding what's normal and what's psychopathology gets influenced by culture and politics.'' This is a stark reminder to us that what is deemed “normal” or “pathological” is shaped by the current values of the society that defines those categories. Perhaps one way that neuroscience can be useful in this context is to help psychiatry become more “objective,” though we will still face challenges with objectivity even when peering inside the brain.
Dr. Pouissant goes on to assert that “contemporary psychiatry is as in the dark about its own biases as the benighted Dr. Cartwright.” In line with this, the diagnosis of schizophrenia today is still rife with implicit anti-Black racism. Black individuals presenting with mental health symptoms are four to five times more likely to be diagnosed with schizophrenia compared to white people. Clinicians are also more likely to overmedicate their Black patients with antipsychotics.
Why are Black people so much more likely to be diagnosed with schizophrenia? While the exact causes are still poorly understood, there are a few hypotheses that may explain this alarming trend. Importantly, there are no “biological” explanations (such as "genetic predispositions") for why Black people are more likely to be misdiagnosed with schizophrenia. Further, race is a social construct and not a biological one.
One explanation is that Black people presenting with mental health issues are systematically misdiagnosed. Studies have shown that Black patients are more likely to be diagnosed with schizophrenia over major depressive disorder, which suggests that clinicians put more emphasis on psychotic rather than depressive symptoms in Black patients. So even when Black patients show similar depressive and manic symptoms as white patients, the diagnosis skews towards schizophrenia over a mood disorder.
Second, it is possible that clinicians may not have the context and cultural understanding to provide the proper diagnosis. Jasmine Mote, PhD, and Daniel Fulford, PhD, in the Approach, Motivation, and Participation (AMP) lab at Boston University explain how this might manifest. Let’s take paranoia as an example, a common symptom in psychotic disorders. Say a patient expresses a belief that their neighbors are watching them at all times and talking about them behind their back. Additionally, the patient mentions that their neighbor called the police on them just because they were outside watering their lawn. As a result, the patient feels that their neighbors are “out to get them.” Is this patient paranoid? The clinician must make a judgement call about whether the thoughts of the patient are “realistic” or not. Perhaps, a clinician may believe that the scenario is unrealistic and that the patient is experiencing paranoid delusions. However, what if the patient is Black and living in a predominantly white neighborhood? This changes the picture dramatically. This hypothetical situation can provide some context for why a clinician might not know how to differentiate genuine paranoia from the real lived experience of the patient; the proper contextual and cultural understanding is key to ensuring a proper diagnosis.
What’s Next?
It seems that Black patients are systematically misdiagnosed with schizophrenia, so what should we do about it? One particularly important issue is that less than one percent of all psychiatrists and only four percent of psychologists identify as Black. Angela Neal-Barrett is a professor in the department of psychological sciences and director of the Program for Research on Anxiety Disorders among African Americans at Kent State University in Ohio. Dr. Neal-Barrett says that Black psychiatrists’ and psychologists’ “voices are critical to our understanding of serious mental illness and disseminating that knowledge into the community.” She builds on this, saying that a community-based participatory research and intervention approach is key to building mental health systems that work to support Black individuals. It is essential to acknowledge the systematic misdiagnosis of Black peoples’ mental illnesses and recognize that systemic bias is at its root. To do this, Dr. Neal Barrett urges that we must invest “years, not months, to build the trust.” Indeed, there are no quick fixes to the systematic misdiagnoses outlined in this article. However, with culturally-competent interventions and more research to better understand mental illness in Black populations we can hopefully ensure better diagnosis and treatment for Black patients in the future.
Senior Editor: Ashlea Morgan
Images curated by Sedona Ewbank